There is tremendous skill and clinical time invested when carrying out an orthokeratology (OrthoK) fit. The ensuing processes are of equal importance to the fitting procedure, including the follow-up schedule and instructional review of care and handling steps associated with a newly established OrthoK wearer. Patient management and follow-up can differ depending on the wearer’s age and if OrthoK use is prescribed for myopia management or myopia correction.
OrthoK Dispense Day
The fitting and dispensing visits may coincide for a diagnostic OrthoK fit. OrthoK lenses taken directly from your fitting set are clean and ready for dispensing; however, they should be evaluated as if they are new each time.
When new OrthoK lenses are dispensed, they should be inspected for smooth edges, cleaned, and conditioned before application on the eye to optimize the first dispense experience. OrthoK lenses are typically plasma treated in the manufacturing process and will arrive from the lab soaking in solution. The purpose of this solution is to pre-condition the new lenses. Package inserts remind fitters that the lens is non-sterile upon arrival and to clean and condition the lens prior to use. Imperfect surface wetting will decrease the quality of vision for the patient when the lens is worn. If a drop of topical anesthetic was used during the OrthoK fitting visit, try to avoid anesthetic during the dispensing visit to set the patient’s expectations for applying the lenses by themselves at home. Also, remind patients that OrthoK lenses are typically manufactured in two different colors (i.e., puRple for the Right eye and bLue for the Left eye) to avoid confusion during the application process. (Figure 3)

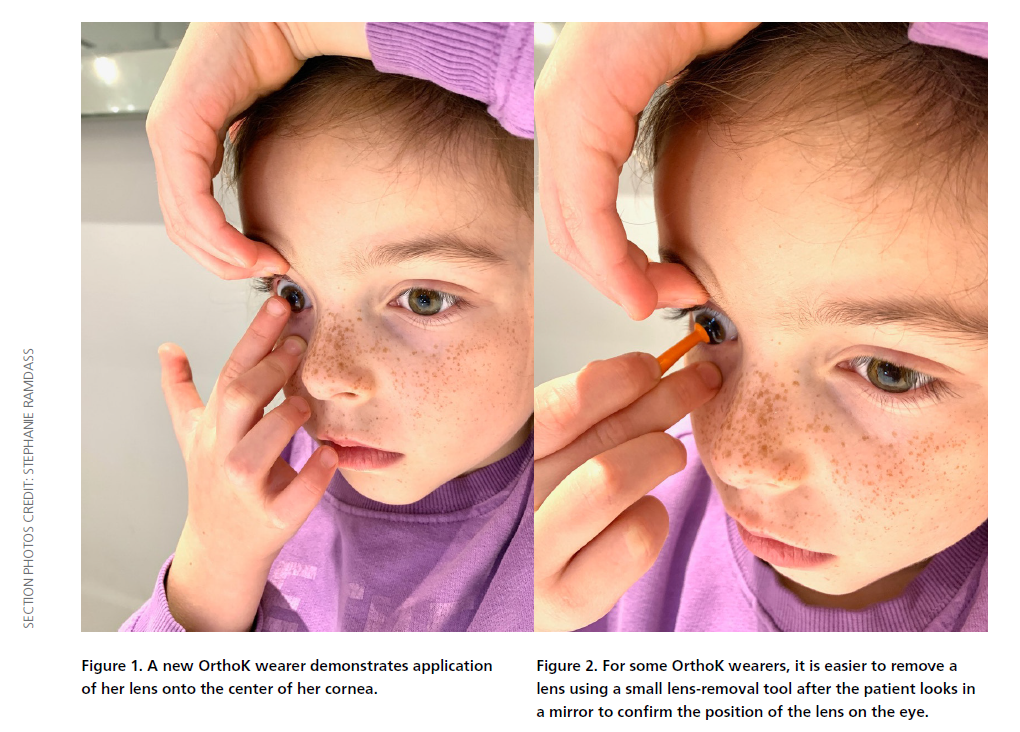
For the youngest OrthoK wearers who may need a caregiver to assist with the application at home, it is imperative to teach this individual how to apply the lenses in the office. Demonstrate that a drop of preservative-free lubricant artificial tears or saline can be used to rinse the lenses prior to application, or a drop of this solution can be placed into the bowl of the lenses prior to application. OrthoK lenses should be placed directly on the “center of the colored part of the eye.” (Figure 1) If it becomes dislodged and ends up on the sclera, instruct the patient and/or caregiver that the eye should part of the eye.” (Figure 1) If it becomes dislodged and ends up on the sclera, instruct the patient and/or caregiver that the eye should look in the direction of the lens in order to recenter it. Alternatively, a drop of solution on the tip of a small lens-removal tool can be used to safely remove the OrthoK lenses. (Figure 2) Patients and/or caregivers should be taught OrthoK lens removal with and without the aid of the lens-removal tool. Care and handling of the lenses should be carefully reviewed at each visit to ensure safety when wearing lenses.
The follow-up visit schedule is determined, whether empirically or diagnostically fit, after the first night of OrthoK overnight wear. This may fall on the night of dispense day or may be at a suitable future date that will allow the patient to return early the following day for the one-day follow-up visit. Depending on the flexibility of both the caregiver’s and the eye care practitioner’s schedules, an early morning appointment may have to be booked outside of regular business hours, either earlier than usual or on the weekend, to minimize the time when lenses are worn in an open-eye state.
OrthoK One-Day Follow-up
For any patient, child, or adult, the first overnight wear can be the most challenging part of OrthoK wear. Initial lens awareness is expected. Lenses should be applied just prior to bed, preferably in the bathroom immediately after handwashing. During OrthoK treatment, the patient should get a full night’s rest, or at least six to eight hours of sleep, for optimal overnight results.
Ideally, a follow-up examination should occur early the next morning, where the caregiver drives the patient or the patient drives themself to your office. If patients are wearing the OrthoK lenses to the office for their first follow-up visit, an early morning visit minimizes the time when lenses are worn in an open-eye state.
Practitioners often debate the significance of OrthoK treatment zone difference analysis on whether patients wear their OrthoK lenses to their office visit the day after their first night of overnight wear or if they don’t. One study assessed the clinical impact of day-one removal of OrthoK.1 A total of 11 subjects (22 eyes) participated in a randomized, crossover study where they were fit with OrthoK lenses according to the manufacturer’s recommendations. During Phase 1, participants wore their OrthoK lenses overnight and removed them at home before their day-one follow-up. These same participants were then washed out of OrthoK wear over a one-to-two week period or until topography maps returned to baseline. Participants resumed treatment again overnight but wore their lenses to the office for the doctor to remove them in-office. When OrthoK lenses were worn to the office, there was a trend for the corresponding tangential difference maps to appear more oval than circular and show a slight double ring effect. (Figure 4A-F) The treatment zone size typically appeared similar in width irrespective of the treatment phase. However, it was of a greater intensity when lenses were worn to the office.

From this pilot study, it appears that one-day treatment in patients undergoing OrthoK can be assessed the morning after overnight wear shortly after awakening, whether they present to the office wearing their lenses or not. As a clinician, it is essential to remember that assessing the ocular health of patients undergoing OrthoK is of the utmost importance. If a patient is dispensed OrthoK lenses and does not present wearing them once throughout their treatment, you may never see them on the eye again. Patients should be encouraged to bring their OrthoK lenses to every visit.
For older patients who require sharp distance acuity to function throughout the day, it may be beneficial to prescribe daily disposable contact lenses in a descending power sequence to correct their vision until the one-week follow-up where the total treatment effect is nearly complete.2 Patients may need additional instruction on the care and handling of the daily disposable lenses as well. Instruct patients to continue with nightly wear of the OrthoK lenses if the dispense day is successful, and schedule them back in one week.
OrthoK Follow-up Schedule
There is no standard protocol for the number of OrthoK follow-ups that must be carried out. Table 1 provides a suggested sequence of appointments centered around maintaining corneal health and reinforcing best practices for patient care and handling, as these steps should be reviewed at each visit. The various tests at each visit can vary, with axial length measurements included for OrthoK patients undergoing myopia management.
OrthoK Evaluation and Lens-Induced Complications
During scheduled follow-up evaluations, ask patients to bring their OrthoK lenses with them. Always inspect for any lens irregularities that might impact the treatment effect or lead to ocular surface complications. Topography maps compared to baseline results, entering visual acuity, residual refraction, best corrected visual acuity, and staining assessment of the ocular surface are key metrics to monitor treatment effect. Review of care and handling procedures can be done quickly and ensure continued patient compliance and health and safety with overnight OrthoK. If patients are enrolled in a myopia management program in your office, quarterly or biannual ocular biometry measurements are helpful benchmarks to monitor treatment efficacy. (Table 1)

Outside of the suggested follow-up schedule, patients and/or caregivers need access to immediate care, or they need to know how to contact the office or the ECP directly, should problems arise.
Care and Handling
Lens cleaning, disinfection, and handling should be reviewed at each visit. Hygiene, especially handwashing, must be stressed. Lens contamination due to care and handling is the number one risk for complications associated with overnight wear of OrthoK lenses.3 For young patients, establishing care routines is essential to help build consistency. Ask patients and/or caregivers to take pictures of their care/handling set-up at home and have them talk through their application, removal, and cleaning steps during follow-up visits. (Figure 5)

Before bed and with clean hands, either a caregiver or patient should remove the OrthoK lenses from the case, one lens at a time. The lens can be rinsed with saline (preferably non-preserved), and then a drop of non-preserved artificial tears can be placed into the bowl of the lens (optional step) and applied. Advise patients not to rub their eyes as this can dislodge the lenses. All solution in the case should be discarded at this time, and the case should be rinsed with saline and allowed to air dry so that it is ready to use again in the morning. Although rare, the lens may fall out or shift while sleeping. If patients wake up in the morning and can see out of each eye, the lenses are correctly in place. After washing their hands, have your patient remove their OrthoK lenses. If they are prone to dryness in the morning, instruct the patient to instill a drop of non-preserved artificial tears into the eye to ensure adequate lens movement before removal with or without the aid of a small lens-remover tool. OrthoK lenses are then disinfected as recommended and placed in the corresponding side of the clean case. Disinfection can be performed with an all-in-one multipurpose GP solution or a hydrogen peroxide-based system.
Back-up/Replacement OrthoK Lenses
It is recommended to have an OrthoK contract in place for each fit. OrthoK is an ongoing process that does not end upon dispense and finalization of lens parameters. Patients and/or caregivers need to understand the responsibilities of an OrthoK wearer and the commitment that goes into year one. This contract should include details regarding a backup pair of lenses, often offered at a discounted rate if a direct duplicate of finalized parameters is ordered and it is within the lab-specified warranty period. Outside of the warranty period, there will be costs associated with broken or replacement lenses. For broken lenses, advise the caregiver/patient that labs want to understand how they broke and often like to keep this information on file. Remind them to take photos of broken lenses and email them to your office for reference. To avoid disrupting the OrthoK treatment process, always encourage patients to have a backup pair. If a wearer has similar topographies and refractive target correction in both eyes, have the patient bring their remaining OrthoK lens to the office and evaluate if it can be worn on each eye on alternating nights to ensure minimal washout and disruption of daily routines until the new lenses arrive.
Annual Management Fees and/or Re-Fit Protocol
At the one-year mark, patients will require an annual exam to ensure that complete ocular health is assessed. An annual management fee can be applied to cover your chair time costs for ongoing OrthoK assessment in year two. This fee may include follow-up visits for the remainder of year two, or it can be independent with subsequent OrthoK follow-ups invoiced à la carte.
The treatment effect of OrthoK lenses may deteriorate as the lenses get older, thus the ECP should recommend that a replacement pair be ordered at this time. A higher than expected residual refraction measured at the one-year visit can easily be remedied with a new set of OrthoK lenses in the habitual parameters. If necessary, a re-fit may be required if a wearer has discontinued lens wear on their own (minimum of three weeks), if lens wear is no longer comfortable, or if the treatment effect is significantly off from the expected outcome.
1 Swanholm A, Ramdass S, Norman, C. Clinical Impact of Day-One Removal of Orthokeratology Contact Lenses (DORO). Poster presented at Vision By Design.
2017.
2 Soni PS, Nguyen TT, Bonanno, J. Overnight Orthokeratology: Refractive and Corneal Recovery After Discontinuation of Reverse-Geometry Lenses. Eye Contact
Lens. 2004. Oct;30(4): 254–262.
3 Liu YM, Xie P. The Safety of Orthokeratology-A Systematic Review. Eye Contact Lens. 2016 Jan;42(1):35-42